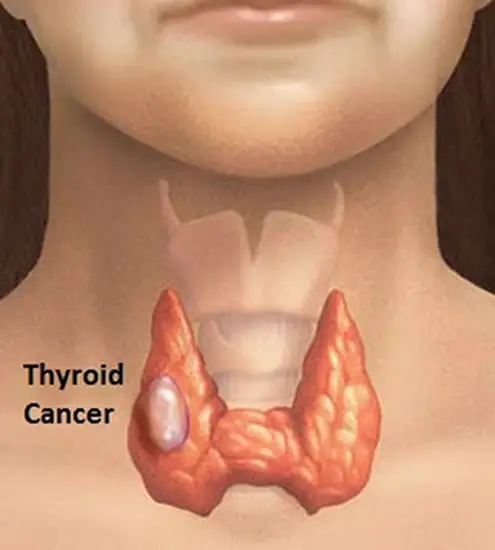
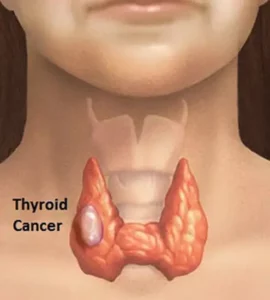
Thyroid cancer is a disease in which malignant (cancer) cells form in the tissues of the thyroid gland. The malignant cells begin multiplying in your thyroid and, once there are enough of them, they form a tumor. It can occur in any age group, although it is most common after age 30. Females are more likely to have thyroid cancer. If it’s caught early, then thyroid cancer is one of the most treatable forms of cancer.
Types of Thyroid Cancer
Thyroid cancer is classified into types based on the kinds of cancerous cells found in the tumor. Your type is determined, when a sample of tissue from your cancer is examined under a microscope.
There are 4 main types of it, and some are more common than others.
Papillary thyroid cancer: It is the most common type, making up about 70% to 80% of all thyroid cancers. Papillary thyroid cancer can occur at any age. It tends to grow slowly and often spreads to lymph nodes in the neck. Even when this cancer have spread to the lymph nodes, it can often be treated successfully and are rarely fatal.
Follicular thyroid cancer. Follicular cancer can spread into your lymph nodes and is also more likely to spread to distant organs, particularly the lungs and bones.
Medullary thyroid cancer (MTC) : It begins in thyroid cells called C cells, which produce the hormone calcitonin, a hormone that helps control the amount of calcium in blood. Elevated levels of calcitonin in the blood can indicate medullary thyroid cancer at a very early stage.
This type of cancer is more difficult to find and treat, There are 2 types of MTC:
- Sporadic MTC: It accounts for about 8 out of 10 cases of MTC, is not inherited (meaning it does not run in families). It occurs mostly in older adults.
- Familial MTC: It is inherited (runs in families). These cancers often develop during childhood or early adulthood and can spread early.
Anaplastic thyroid cancer: It is the most advanced and aggressive thyroid cancer and the least likely to respond to treatment. It is very rare and is found in less than 2% of patients with thyroid cancer. This cancer often spreads quickly into the neck and to other parts of the body, and is very hard to treat.
Other rare types: Other very rare types of cancer that start in the thyroid includes:
- Thyroid lymphoma: which begins in the immune system cells of the thyroid.
- Thyroid sarcoma: which begins in the connective tissue cells of the thyroid.
Symptoms of Thyroid Cancer
Thyroid cancer may not cause early signs or symptoms. That’s because there are very few symptoms in the beginning. Signs or symptoms may occur as the tumor gets bigger. Check with your doctor if you have any of the following:
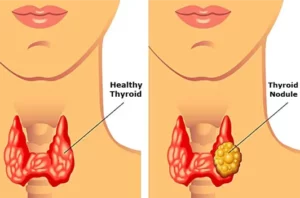
- A lump (nodule) in the neck.
- Trouble breathing.
- Pain when swallowing.
- Hoarseness.
What cause Thyroid Cancer?
It is more common in people who have a history of exposure to high doses of radiation, have a family history of thyroid cancer, and are older than 40 years of age. However, for most patients, there is no specific reason why they get it.
Diagnosing Thyroid Cancer
Thyroid cancer may be diagnosed after a person goes to a doctor because of symptoms, or it might be found during a routine physical exam or other tests. If there is a reason to suspect you might have thyroid cancer, your doctor will use one or more tests to confirm the diagnosis.
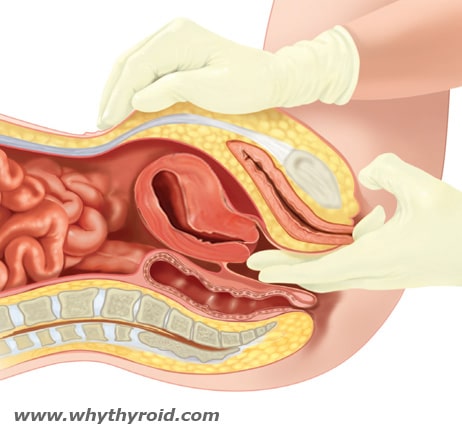
Physical Exam: Your doctor will examine your neck to feel for physical changes in your thyroid, such as thyroid nodules. He or she may also ask about your risk factors, such as past exposure to radiation and a family history of thyroid tumors.
Blood tests: Blood tests are not used to find thyroid cancer. But they can help show if your thyroid is working normally, which may help the doctor decide what other tests may be needed. They can also be used to monitor certain cancers.
Calcitonin level in the blood: Calcitonin is a hormone that helps control how the body uses calcium. It is made by C cells in the thyroid, the cells that can develop into medullary thyroid cancer (MTC). If MTC is suspected or if you have a family history of the disease, blood tests of calcitonin levels can help look for MTC. Because calcitonin can affect blood calcium levels, these may be checked as well.
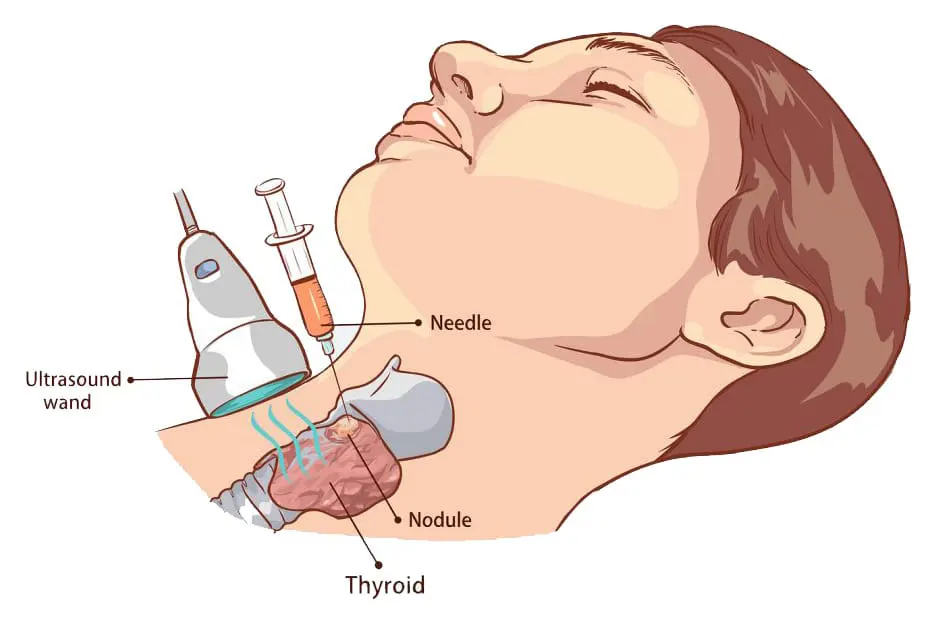
Ultrasound imaging: Ultrasound uses high-frequency sound waves to create pictures of body structures. To create an image of the thyroid, the ultrasound transducer is placed on your lower neck. The image of your thyroid and any nodules, even those you can’t feel, will show up on a computer screen.
This test can help determine if a lump is filled with fluid or if it’s solid. A solid one is more likely to have cancerous cells, but you’ll still need more tests to find out. The ultrasound will also show the size and number of nodules on your thyroid.
Thyroid Biopsy: The actual diagnosis of thyroid cancer is made with a biopsy, in which cells from the suspicious area are removed and looked in the laboratory for cancer cells.
If your doctor thinks a biopsy is needed, he/she will do (Fine needle aspiration (FNA)) biopsy, in which a small, thin needle is used to take a little sample from the lump, and maybe other places around it. This type of biopsy can sometimes be done in your doctor’s office or clinic. You won’t need any recovery time afterward.
After he gets the sample, the doctor will send the sample to a lab for testing.
Genetic testing: Based on your family history, your doctor might order genetic testing to find out if you have any genes that make you more likely to get cancer. It can also show genetic changes that could be a sign of certain types of thyroid cancer.
Radioiodine scan: This can be used to help determine if someone with a lump in the neck might have thyroid cancer. For this test, a small amount of radioactive iodine is swallowed (usually as a pill) or injected into a vein. Over time, the iodine is absorbed by the thyroid gland (or thyroid cells anywhere in the body). A special camera is used several hours later to see where the radioactivity is.
CT Scan (Computed tomography): Computed tomography, commonly called a CT scan or CAT scan, uses special X-rays to give your doctor a look inside of your body. It can show the size and location of thyroid cancer and whether it has spread to other parts of your body.
MRI Scan (Magnetic resonance imaging): A MRI can be used to look for cancer in the thyroid, or cancer that has spread to nearby or distant parts of the body. MRI can provide very detailed images of soft tissues such as the thyroid gland.
PET Scan (Positron emission tomography): This test uses small amounts of radioactive material, called radiotracers, a special camera, and a computer to look at your organs and tissue. A PET scan looks at changes on the cellular level. It may be able to detect the cancer in a very early state and check for cancer spread.
Treatments of Thyroid Cancer
Your thyroid cancer treatment depend on the type and stage of your thyroid cancer. It also depends on your age, general health, and other things that are unique to you. The treatment options for thyroid cancer might include:
Surgery: Surgery is the main treatment, in nearly every case of thyroid cancer. If thyroid cancer is diagnosed by biopsy, surgery to remove the tumor and all or part of the remaining thyroid gland is usually recommended. Operations used to treat thyroid cancer include:
- Lobectomy (Removing a portion of the thyroid gland): During this operation, the surgeon removes half of the thyroid. It might be recommended if you have a slow-growing thyroid cancer in one part of the thyroid and no suspicious nodules in other areas of the thyroid.
- Thyroidectomy (Removing all or most of the thyroid gland): It is a surgery to remove the thyroid gland. If the entire thyroid gland is removed, it is called a total thyroidectomy. Sometimes the surgeon may not be able to remove the entire thyroid. If nearly all of the gland is removed, it is called a near-total thyroidectomy.
- Lymph node removal: If cancer has spread to nearby lymph nodes in the neck, these will be removed at the same time surgery is done on the thyroid.
Complications are less likely to happen when your operation is done by an experienced thyroid surgeon. However, thyroid surgery still carries a risk of bleeding and infection. Damage to your parathyroid glands also can occur during surgery, which can lead to low calcium levels in your body.
There’s also a risk that the nerves connected to your vocal cords might not work normally after surgery, which can cause vocal cord paralysis, hoarseness, voice changes or difficulty breathing.
Radioactive Iodine Therapy: The thyroid gland and most thyroid cancers absorb iodine. Radioactive iodine (RAI) ablation is used to destroy any thyroid tissue that’s left after a thyroidectomy. The Radioactive Iodine collects mainly in thyroid cells, where the radiation destroys the thyroid gland and any other thyroid cells (including cancer cells), with little effect on the rest of your body.
The level of radiation in this treatment is far higher than what is used in a radioiodine scan.
Side effects of RAI treatment may include:
- Dry mouth
- Nausea and vomiting
- Neck tenderness and swelling
- Taste changes
Most of the radioactive iodine leaves your body in your urine in the first few days after treatment. You will be given instructions on how to protect others from radiation exposure and how long you need to take these precautions. These instructions may vary slightly by treatment center. Be sure you understand the instructions before you leave the hospital.
External beam radiation therapy: Radiation therapy can also be given externally using a machine that aims high-energy beams, at precise points on your body to destroy cancer cells or slow their growth. During treatment, you lie still on a table while a machine moves around you.
External beam radiation therapy is often used for cancers that continues to grow even after radioactive iodine treatment and have spread beyond the thyroid. Radiation therapy may also be recommended after surgery if there’s an increased risk that your cancer will recur.
Chemotherapy (chemo): Chemotherapy uses anti-cancer drugs that are injected into a vein or are taken by mouth. Chemotherapy is systemic therapy, which means that the drug enters the bloodstream and travels throughout the body to reach and kill cancer cells.
Chemo isn’t commonly used in the treatment of thyroid cancer, but it’s sometimes recommended for people with anaplastic thyroid cancer. Chemotherapy may be combined with external beam radiation therapy.
Chemotherapy has side effects, but your doctor will help you to manage them.
Targeted drug therapy: It is a newer treatment that targets only certain parts of cancer cells, to slow or stop growth. This is normally taken in pill form. It’s typically used in advanced thyroid cancer. Usually, there are fewer side effects than with chemotherapy.
Follow-up care
Follow-up is needed to check for cancer recurrence or spread, as well as possible side effects of certain treatments. It’s important for all thyroid cancer survivors to let their health care team know about any new symptoms or problems, because they could be caused by the cancer coming back or by a new disease or second cancer.
Most people do very well after treatment, but follow-up care is very important since most thyroid cancers grow slowly and can recur even 10 to 20 years after initial treatment.
Thyroid Cancer Prognosis
Overall, the prognosis of differentiated thyroid cancer is excellent, especially for patients younger than 45 years of age and those with small cancers. Patients with papillary thyroid cancer, who have a primary tumor that is limited to the thyroid gland have an excellent outlook. For patients older than 45 years of age, or those with larger or more aggressive tumors, the prognosis remains very good, but the risk of cancer recurrence is higher.
The prognosis may not be quite as good in patients whose cancer is more advanced and cannot be completely removed with surgery or destroyed with radioactive iodine treatment. However, these patients often are able to live a long time and feel well, despite the fact that they continue to live with cancer.
Furthermore, it is important to talk to your doctor about your individual profile of cancer and expected prognosis. It will be necessary to have lifelong monitoring, even after successful treatment.
| Related Topics… | |
|
|
|
Thyroid Nodules Click to Read… |
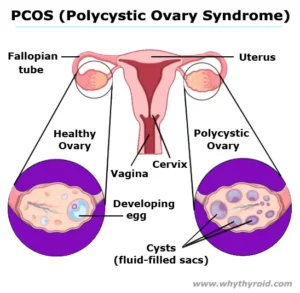
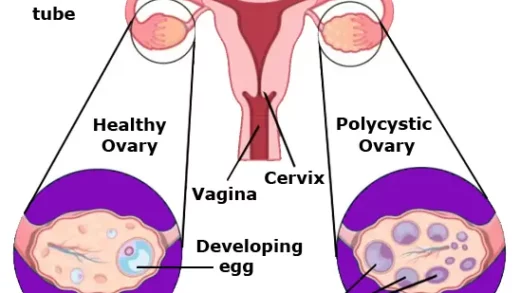
Polycystic Ovary Syndrome (PCOS) Click to Read… |
6 Sources






I genuinely thank you for your information. The article has truly peaked my interest.
Thank you for your valuable comment. Keep reading. 🙂
Great post. I am experiencing some of these issues as well..
Thank you for your valuable comment. Keep reading. 🙂
I’m really loving the theme of this
site. It’s simple, yet effective.
I must say you’ve done a excellent job with this.
Additionally, the blog loads super fast for me on Opera.
Exceptional Blog!
Thank you for your valuable comment. Keep reading. 🙂